
Appreciative Communication Styles for Social Workers
Prepared by: PP-15 Johanniter Austria Research and Education – (JOAFG), Austria
Communication is an essential part of human life. At the same time, it is a highly complex and heterogeneous phenomenon, that consists of many different aspects. Communication can be verbal, paraverbal (i.e. how you say the words you say) and non-verbal. This training programme focuses explicitly on interpersonal communication.
Lesson #1: Basics and Useful Information on Communication
In order to communicate properly and purposeful, a basic understanding of the process of communication and communication skills is necessary.
1.1 Basic Overview
When people meet each other, they also communicate. In verbal or nonverbal form (i.,e. behaviour), messages are exchanged. It is common knowledge by now that the meaning of a message for a receiver depends on the content, on the relationship to the sender, on the sender and receiver themselves, and on the context. At the beginning of the 1980s, Friedemann Schulz von Thun developed his concept of the four sides of a message (see. Fig. 1), which is still popular today.
Figure 1: Four-sides-model by F. Schulz von Thun © RWTH Aachen
According to Schulz von Thun, a message has four aspects or sides. It has factual information, a relationship component, a self-revelation component, and an appeal component.
The factual information is encoded in some form by the sender of the message and must be decoded again by the receiver. Such encodings can be language, symbols, or other forms of signs (e.g., sign language). In order to be able to transmit and receive the factual content reliably, the sender and receiver must necessarily have the same character set. If the sender and receiver only speak and understand different languages, a transmitted message cannot be decoded or translated by the receiver. If the character sets of the sender and receiver do not match, misunderstandings will occur. These can go so far that the recipient does not understand the content at all. This can already occur when individual words are understood differently or not at all. Thus it would be possible to make a message difficult, if not unreadable, by the extensive use of foreign words sentences, undefined abbreviations, etc. (Lubienetzki & Schüler-Lubienetzki, 2020).
The relationship component revolves around the question of how sender and receiver define their relationship, as words and behavior are adapted accordingly. If two friends meet and one greets the other with the sentence "Well, my boy, how are you?", this sentence is presumably congruent with the friendly relationship of the two. If the relationship definition of the sender and receiver match, the probability is high that the message will be understood as it is meant. If the recipient of the message has a different definition of the relationship, there will be irritations and misunderstandings (Lubienetzki & Schüler-Lubienetzki, 2020).
Through self-revelation, as the word implies, a person always shows something about themselves. The language or the way someone expresses themselves for example reveals something about their linguistic environment or where they come from. A person's behavior also gives clues about how they are feeling at the moment (e.g. is the person excited or calm, tense or relaxed?). Behavior reveals our own internalized attitude with which we approach another person. Even if a person tries to suppress or cover up their attitude or emotions, something comes across to us. Sometimes it is only a slight feeling of irritation (Lubienetzki & Schüler-Lubienetzki, 2020).
The fourth side of a message is the appeal, which means that there is usually an intention behind a message. Hardly anything is said 'just so’. The exact intention behind a message can be stated openly or hidden. In the second case, the sender could be trying to manipulate the receiver.
Von Thun’s model shows that how a person communicates has effects on their message. If you can communicate your ideas clearly and concisely, the other person will retain the meaning well and understand your message. Still, two people who speak the same language and have the same vocabulary can, but do not necessarily have to, communicate successfully. The public political debate, for example, shows us every day that communication is more than the mere exchange of verbal and nonverbal strings (Lubienetzki & Schüler-Lubienetzki, 2020).
Another commonly known model of human communication are the five axioms according to Paul Watzlawick (see Fig 2). An axiom is understood here firstly as a principle or a valid truth recognized as absolutely correct, which does not require proof, and secondly as a non-derived statement of a scientific field, from which other statements are deduced (Lubienetzki & Schüler-Lubienetzki, 2020).
The first axiom is ‘One cannot not communicate.’ For the model, this axiom means that communication is continuous. The participants express themselves verbally and/or nonverbally and behave in the communication process without interruption. Through this, the communication participants influence each other at every moment. Communication is always cause and effect, it is therefore circular.
Figure 2: 5 Axioms according to Paul Watzlawick © Smarter Together (2021)
The second axiom formulated by Watzlawick is 'Any communication has a content as well as a relationship aspect', such that the latter determines the former. This axiom posits the relationship between two people as determining communication. The range of meaning of sentences such as "You look good today." can range from the highest praise to the deepest insult through the relationship between two people (Lubienetzki & Schüler-Lubienetzki, 2020).
Figuratively speaking, communication is circular, that is, without beginning and end. People who are in a relationship with each other communicate, and everything that has happened in the relationship so far is part of it. Nevertheless, people set their personal starting points in communication, from which their communicative behavior then depends. The corresponding axiom for this is: ‘We usually experience our behavior as a reaction.’
Watzlawick refers to the way in which actors interact as modalities. The axiom for this is formulated as ‘Communication is also non-verbal (analogue & digital).’ The digital strand (language, signs, symbols, etc.) is primarily used to convey factual content. This modality is not very accessible for relationships and feelings. The level of the relationship is illuminated via the analog strand (facial expressions, gestures, behavior, etc.). As precise as digital expressions are (e.g., in the form of linguistic expressions), analog ones are imprecise. Most of the time, these are ambiguous. A smile can express kindness or contempt. There are tears of joy and of sadness. There is no complete certainty in communication that messages will reach the other person. However, by combining digital and analog modalities, the intended message can be made clear. The overall picture emerges on all channels (Lubienetzki & Schüler-Lubienetzki, 2020).
The fifth and last axiom is ‘Communication is symmetric or complementary.’ If the communication is symmetrical, this means that both communication partners strive for equality and interact accordingly. They mirror each other, so to speak. Strength is met with strength, weakness is met with weakness or hardness with hardness etc. Complementary communication shows a different matching behavior, which is about a coordinated and expected difference. Such complementary relationships arise for example between teachers and students, mother and child, or managers and employees. What the expectations are in such relationships depends, among other things, on the cultural background. If the expectations of complementarity are not fulfilled, this leads to disruptions in communication. For example, if an older person in Japan is not treated with emphatic respect by a younger person, this circumstance can significantly impair communication or even make it impossible. The communication partners simply do not understand each other. Regardless of whether the communication situation is symmetrical or complementary, it is crucial for the course of communication whether the partners have the same or a different definition of their relationship. Deviations in the definition can lead to disruptions. (Lubienetzki & Schüler-Lubienetzki, 2020).
1.2 Communication Styles
In this training programme we define a communication style as “the characteristic way a person sends verbal, paraverbal, and nonverbal signals in social interactions denoting (a) who he or she is or wants to (appear to) be, (b) how he or she tends to relate to people with whom he or she interacts, and (c) in what way his or her messages should usually be interpreted” (de Vries et al., 2009).
Communication styles change from person to person. During the process of communication, a person may invoke several channels or modes or methods to convey a message. But the process of communication doesn’t only depend on the source producing or relaying information, it also equally depends on the communication method and the manner in which the receiver understands the message. “Communication styles play not only a role in personal relations but also in relations between teachers and pupils, doctors and patients, leaders and subordinates, consultants and clients, politicians and the public” (de Vries et al., 2013).
Lesson #2: Basics of De-escalation ("First Aid" in Conflict Situations)
Having effective communication skills is very important in professional, as well as personal life. Especially in high stress and/ or conflict situations, clear communication is essential. In some job areas however, such as emergency or health related services, improper communication skills may lead to confusing or incomplete instructions, which can have very serious negative consequences. Here, excellent communication skills are not just beneficial, but can literally save lives by communicating accurate information clearly to the patient or other target groups.
An important topic in conflict situations is de-escalation, which is the communicative prevention of conflict and means avoiding a mutual running up of emotions and aggression. In emergency or health related services, there is a particular need to thoroughly address the emergence of violence and aggression and to learn the best way to deal with aggressive behaviours, because when working with patients, the likelihood of tense situations occurring is significantly increased. In the course of every illness, care or support, there are phases in which aggression can arise. Fears, loss of autonomy and self-esteem, existential worries, personal crises, pain, anger (at oneself or at others), etc. put a strain on the patients. At the same time, they are inwardly more vulnerable, helpless and sensitive. This mixture creates an inner field of tension, in which the affected person can become can react aggressively even to trivial things. Especially people with a lack of insight (e.g. small children, mentally ill people) may not understand the sense and the necessity of measures to improve their health or to protect them and therefore experience these measures as violence directed against themselves and their needs, which could result in aggressive counter-reactions (Wesuls et al., 2005).
There are several communicative strategies in de-escalation that significantly increase the chance of resolving the conflict without violence. In addition to the content level of communication, i.e. the actual choice of words, both the paraverbal level and the nonverbal level play a very important role in de-escalation. The voice and the body language have a very strong effect and here the bridge to the inner state closes again. It is much easier to appear convincing when you are convinced.
De-escalation is focused on understanding, interpreting, changing and preventing aggression wherever it occurs. De-escalating work can take place on many different levels, e.g., in preventing the emergence of aggression, in calming conversation with a tense patient, in resolving conflicts without defeat, or even in restraint that is carried out in a humane and patient-friendly manner and thus prevents further brachial aggression on the part of the patient. De-escalating work is possible at every stage of the development and escalation of aggression (Wesuls et al., 2005).
In contact with an aggressive patient, one must become more aware of the professionalism of the relationship. While in private relationships one can react to aggression intuitively, spontaneously and without reflection, dealing with aggression in the professional relationship with the patient must be planned, goal-oriented and reflected.
Wesuls et al. (2005) created 12 basic rules of de-escalation:
Figure 3: 12 Basic Rules of De-escalation © Wesuls et al. (2005)
Communication is an essential part of human life. At the same time, it is a highly complex and heterogeneous phenomenon, that consists of many different aspects. Communication can be verbal, paraverbal (i.e. how you say the words you say) and non-verbal. This training programme focuses explicitly on interpersonal communication.
Lesson #1: Basics and Useful Information on Communication
In order to communicate properly and purposeful, a basic understanding of the process of communication and communication skills is necessary.
1.1 Basic Overview
When people meet each other, they also communicate. In verbal or nonverbal form (i.,e. behaviour), messages are exchanged. It is common knowledge by now that the meaning of a message for a receiver depends on the content, on the relationship to the sender, on the sender and receiver themselves, and on the context. At the beginning of the 1980s, Friedemann Schulz von Thun developed his concept of the four sides of a message (see. Fig. 1), which is still popular today.
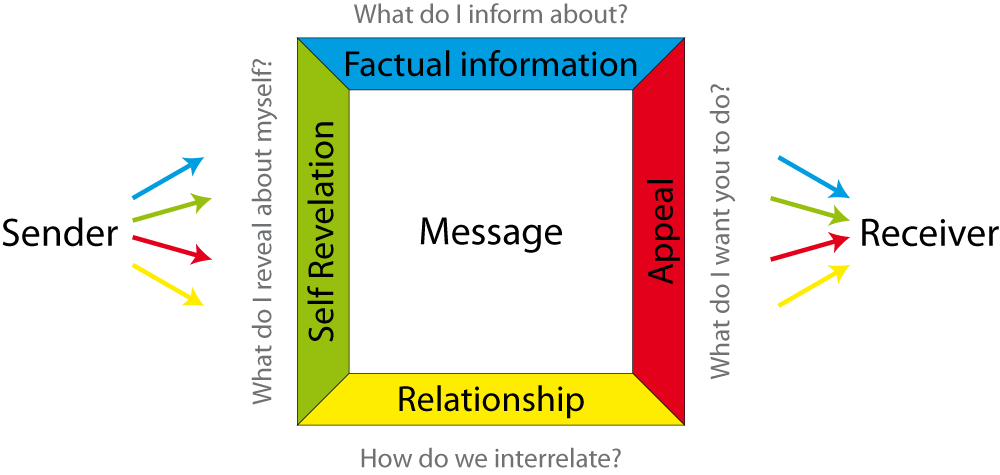
Figure 1: Four-sides-model by F. Schulz von Thun © RWTH Aachen
According to Schulz von Thun, a message has four aspects or sides. It has factual information, a relationship component, a self-revelation component, and an appeal component.
The factual information is encoded in some form by the sender of the message and must be decoded again by the receiver. Such encodings can be language, symbols, or other forms of signs (e.g., sign language). In order to be able to transmit and receive the factual content reliably, the sender and receiver must necessarily have the same character set. If the sender and receiver only speak and understand different languages, a transmitted message cannot be decoded or translated by the receiver. If the character sets of the sender and receiver do not match, misunderstandings will occur. These can go so far that the recipient does not understand the content at all. This can already occur when individual words are understood differently or not at all. Thus it would be possible to make a message difficult, if not unreadable, by the extensive use of foreign words sentences, undefined abbreviations, etc. (Lubienetzki & Schüler-Lubienetzki, 2020).
The relationship component revolves around the question of how sender and receiver define their relationship, as words and behavior are adapted accordingly. If two friends meet and one greets the other with the sentence "Well, my boy, how are you?", this sentence is presumably congruent with the friendly relationship of the two. If the relationship definition of the sender and receiver match, the probability is high that the message will be understood as it is meant. If the recipient of the message has a different definition of the relationship, there will be irritations and misunderstandings (Lubienetzki & Schüler-Lubienetzki, 2020).
Through self-revelation, as the word implies, a person always shows something about themselves. The language or the way someone expresses themselves for example reveals something about their linguistic environment or where they come from. A person's behavior also gives clues about how they are feeling at the moment (e.g. is the person excited or calm, tense or relaxed?). Behavior reveals our own internalized attitude with which we approach another person. Even if a person tries to suppress or cover up their attitude or emotions, something comes across to us. Sometimes it is only a slight feeling of irritation (Lubienetzki & Schüler-Lubienetzki, 2020).
The fourth side of a message is the appeal, which means that there is usually an intention behind a message. Hardly anything is said 'just so’. The exact intention behind a message can be stated openly or hidden. In the second case, the sender could be trying to manipulate the receiver.
Von Thun’s model shows that how a person communicates has effects on their message. If you can communicate your ideas clearly and concisely, the other person will retain the meaning well and understand your message. Still, two people who speak the same language and have the same vocabulary can, but do not necessarily have to, communicate successfully. The public political debate, for example, shows us every day that communication is more than the mere exchange of verbal and nonverbal strings (Lubienetzki & Schüler-Lubienetzki, 2020).
Another commonly known model of human communication are the five axioms according to Paul Watzlawick (see Fig 2). An axiom is understood here firstly as a principle or a valid truth recognized as absolutely correct, which does not require proof, and secondly as a non-derived statement of a scientific field, from which other statements are deduced (Lubienetzki & Schüler-Lubienetzki, 2020).
The first axiom is ‘One cannot not communicate.’ For the model, this axiom means that communication is continuous. The participants express themselves verbally and/or nonverbally and behave in the communication process without interruption. Through this, the communication participants influence each other at every moment. Communication is always cause and effect, it is therefore circular.

Figure 2: 5 Axioms according to Paul Watzlawick © Smarter Together (2021)
The second axiom formulated by Watzlawick is 'Any communication has a content as well as a relationship aspect', such that the latter determines the former. This axiom posits the relationship between two people as determining communication. The range of meaning of sentences such as "You look good today." can range from the highest praise to the deepest insult through the relationship between two people (Lubienetzki & Schüler-Lubienetzki, 2020).
Figuratively speaking, communication is circular, that is, without beginning and end. People who are in a relationship with each other communicate, and everything that has happened in the relationship so far is part of it. Nevertheless, people set their personal starting points in communication, from which their communicative behavior then depends. The corresponding axiom for this is: ‘We usually experience our behavior as a reaction.’
Watzlawick refers to the way in which actors interact as modalities. The axiom for this is formulated as ‘Communication is also non-verbal (analogue & digital).’ The digital strand (language, signs, symbols, etc.) is primarily used to convey factual content. This modality is not very accessible for relationships and feelings. The level of the relationship is illuminated via the analog strand (facial expressions, gestures, behavior, etc.). As precise as digital expressions are (e.g., in the form of linguistic expressions), analog ones are imprecise. Most of the time, these are ambiguous. A smile can express kindness or contempt. There are tears of joy and of sadness. There is no complete certainty in communication that messages will reach the other person. However, by combining digital and analog modalities, the intended message can be made clear. The overall picture emerges on all channels (Lubienetzki & Schüler-Lubienetzki, 2020).
The fifth and last axiom is ‘Communication is symmetric or complementary.’ If the communication is symmetrical, this means that both communication partners strive for equality and interact accordingly. They mirror each other, so to speak. Strength is met with strength, weakness is met with weakness or hardness with hardness etc. Complementary communication shows a different matching behavior, which is about a coordinated and expected difference. Such complementary relationships arise for example between teachers and students, mother and child, or managers and employees. What the expectations are in such relationships depends, among other things, on the cultural background. If the expectations of complementarity are not fulfilled, this leads to disruptions in communication. For example, if an older person in Japan is not treated with emphatic respect by a younger person, this circumstance can significantly impair communication or even make it impossible. The communication partners simply do not understand each other. Regardless of whether the communication situation is symmetrical or complementary, it is crucial for the course of communication whether the partners have the same or a different definition of their relationship. Deviations in the definition can lead to disruptions. (Lubienetzki & Schüler-Lubienetzki, 2020).
1.2 Communication Styles
In this training programme we define a communication style as “the characteristic way a person sends verbal, paraverbal, and nonverbal signals in social interactions denoting (a) who he or she is or wants to (appear to) be, (b) how he or she tends to relate to people with whom he or she interacts, and (c) in what way his or her messages should usually be interpreted” (de Vries et al., 2009).
Communication styles change from person to person. During the process of communication, a person may invoke several channels or modes or methods to convey a message. But the process of communication doesn’t only depend on the source producing or relaying information, it also equally depends on the communication method and the manner in which the receiver understands the message. “Communication styles play not only a role in personal relations but also in relations between teachers and pupils, doctors and patients, leaders and subordinates, consultants and clients, politicians and the public” (de Vries et al., 2013).
Lesson #2: Basics of De-escalation ("First Aid" in Conflict Situations)
Having effective communication skills is very important in professional, as well as personal life. Especially in high stress and/ or conflict situations, clear communication is essential. In some job areas however, such as emergency or health related services, improper communication skills may lead to confusing or incomplete instructions, which can have very serious negative consequences. Here, excellent communication skills are not just beneficial, but can literally save lives by communicating accurate information clearly to the patient or other target groups.
An important topic in conflict situations is de-escalation, which is the communicative prevention of conflict and means avoiding a mutual running up of emotions and aggression. In emergency or health related services, there is a particular need to thoroughly address the emergence of violence and aggression and to learn the best way to deal with aggressive behaviours, because when working with patients, the likelihood of tense situations occurring is significantly increased. In the course of every illness, care or support, there are phases in which aggression can arise. Fears, loss of autonomy and self-esteem, existential worries, personal crises, pain, anger (at oneself or at others), etc. put a strain on the patients. At the same time, they are inwardly more vulnerable, helpless and sensitive. This mixture creates an inner field of tension, in which the affected person can become can react aggressively even to trivial things. Especially people with a lack of insight (e.g. small children, mentally ill people) may not understand the sense and the necessity of measures to improve their health or to protect them and therefore experience these measures as violence directed against themselves and their needs, which could result in aggressive counter-reactions (Wesuls et al., 2005).
There are several communicative strategies in de-escalation that significantly increase the chance of resolving the conflict without violence. In addition to the content level of communication, i.e. the actual choice of words, both the paraverbal level and the nonverbal level play a very important role in de-escalation. The voice and the body language have a very strong effect and here the bridge to the inner state closes again. It is much easier to appear convincing when you are convinced.
De-escalation is focused on understanding, interpreting, changing and preventing aggression wherever it occurs. De-escalating work can take place on many different levels, e.g., in preventing the emergence of aggression, in calming conversation with a tense patient, in resolving conflicts without defeat, or even in restraint that is carried out in a humane and patient-friendly manner and thus prevents further brachial aggression on the part of the patient. De-escalating work is possible at every stage of the development and escalation of aggression (Wesuls et al., 2005).
In contact with an aggressive patient, one must become more aware of the professionalism of the relationship. While in private relationships one can react to aggression intuitively, spontaneously and without reflection, dealing with aggression in the professional relationship with the patient must be planned, goal-oriented and reflected.
Wesuls et al. (2005) created 12 basic rules of de-escalation:

Figure 3: 12 Basic Rules of De-escalation © Wesuls et al. (2005)
1. Resist the beginnings!
De-escalating intervention should take place as soon as the first signs of discontent, tension, restlessness or irritability in a patient appear. Very often, these first signs of impending escalation are not noticed, or not taken seriously. The many pressing routine tasks and corresponding time pressure tempt people to wait and see. The later the reaction, the more difficult the de-escalation and the lower the chance of an injury-free outcome. The sooner you react, the better.
2. Think about your own safety!
Check well whether you think the situation can be handled by you alone and do not be afraid to involve colleagues (never play the hero!). Coming into contact with a high-strung patient always means putting yourself in a dangerous situation. It is therefore important to observe safety measures and rules of conduct that ensure your own safety in contact with the patient.
3. Remove onlookers!
It is important to also consider the dangers for people who are not (yet) directly involved, but who often enjoy all too happy to watch the spectacle. Colleagues should remove onlookers carefully but firmly. De-escalation is much more difficult in front of a platform of onlookers because the patient will not show his background feelings, hardships or problems, but wants to appear strong and powerful.
4. Keep calm!
Of course, in a highly tense situation, you yourself are tense, agitated and fearful. Practice shows that a person who knows how to calm themselves also exerts a calming effect on the patient. Most important is the contact with one's own breathing, which in stressful situations tends to hyperventilate or falter. One breathes in more air than one breathes out. You can counteract this by consciously exhaling completely again and again and letting the breathing reflex do the inhaling. Directing the inhaled air into the abdomen has a calming effect. One's own increasing body tension (mostly in the arms, shoulders or back) can be counteracted by consciously letting go of individual parts of the body.
5. The tense patient needs a contact person!
Never confront the patient with several colleagues at the same time, if you still see a chance of a non-violent outcome to the situation. Verbal de-escalation attempts should only ever be carried out by one person, colleagues should not be visible or appear uninvolved in the background (e.g., in casual conversation with each other). If several people are looking at and observing the patient, this frightens and unsettles the patient. They may feel pressured and their tension increases. Instead, it is important to keep all possible stimuli away from the patient and let them feel like they have an overview of the situation and are able to control it. Contact with the patient should be made by the person who has the best chance of being accepted at the moment of the event and who is most confident in terms of their daily form. Neither the professional group nor the hierarchical position is decisive!
6. Pay attention to your body language, facial expressions, gestures and voice!
The patient must not feel challenged or threatened by your posture. Men in particular run the risk of unconsciously wanting to radiate strength and dominance in tense situations and make their upper arms and chest look powerful. Rather, approach an aggressive patient as you would a frightened animal (e.g., a horse or deer) with which you want to establish contact. Observe and reflect on your facial expressions and gestures. They should be used sparingly and serve to reassure the patient. Hectic movements or sweeping gestures may be perceived as a threat or further irritation.
7. Make eye contact!
It is important to repeatedly make brief eye contact with the patient. However this must not seem intrusive, observing or staring. Also look away from the patient from time to time, so as not to create a feeling of being crowded and watched. However, never take your eyes completely off the patient. At least out of the corner of the eye you must still be able to perceive their movements. Completely turning away carries the risk of a sudden attack with no possibility of defense.
8. Never try to control or dominate the patient!
Instead, you should concentrate on controlling the situation including precautions, your posture, and your breathing. If you are inwardly controlled and in command of the situation, you can meet the patient's agitation with more tolerance and calm confidence. Power struggles between you and the patient must be avoided at all costs. It is completely irrelevant who is currently right. Calmly agree with the patient's point of view - even against your conviction (except in the case of delusions). However do not go so far as to make promises that cannot be kept afterwards. Do not urge the patient to do anything, e.g., sit down or calm down. Avoid continuous appeals.
9. Do not let yourself be provoked or hit by verbal aggression!
The aggressive patient has "fool's liberty" at the moment of a threatening escalation, as long as they do not become violent. Any insults or devaluations should simply be ignored and not used as a reason for threats, admonishments or personal reactions. The patient does not really mean you personally at the moment. They want to prevent anyone from getting too close to them or are angry at the institution of which you are the representative at the moment.
10. Avoid even provocative terms, reproaches, admonitions or threats!
Reproaching a high-strung patient for being very aggressive at the moment can be the straw that breaks the camel's back. Exhortations to calm down or threats of consequences will also make the situation useless as a de-escalation partner for the patient. Instead, signal your concern for the patient, express that you want to and, most importantly, that you are interested in what is bothering, stressing, upsetting or makes them angry.
11. Appreciative attitude!
Meet the high-strung patient with respect, sincerity and empathy. Imagine that you are dealing with a person in great inner distress in front of you, who is in danger of losing control, harming themselves and others. This patient deserves to be supported in their exhausting struggle for control and in their inner tension and despair.
12. Work out needs and feelings!
Try to find out the current reason for the patient's agitation and tension, either by your perception or by asking careful questions. Anticipate or guess the patient's possible needs and match your actions and procedures to them. Offering a drink, a walk, or other distractions, may be beneficial. Show the patient that you are willing to do something for them, even though you may not be able to meet what they ask of you. However, be careful not to overwhelm the patient with questions or offers. A highly strung patient needs much more time to think about a question or offer. Allow them this time and only bring up further questions or offers after the previous ones have been answered or rejected.
Lesson #3: Tips for Communicating with a Person with Dementia
Dementia is a progressive condition that affects cognition and functioning (e.g. memory loss, difficulty communicating or finding words, confusion and disorientation). Most patients with dementia also experience psychological changes such as personality changes, depression, anxiety and/ or inappropriate behaviour (Walaszek, 2020) (see Fig. 4).
Figure 4: Common Symptoms of Dementia © neofect (2021)
Persons affected by dementia often battle with feelings of fear and insecurity, such as fearing memory loss and thinking skills or ‘loosing who they are’. At later stages, they may not understand what's going on or they feel they're not in control of what's happening around them or to them. All of this can affect their behavior.
These symptoms may make it challenging to communicate with a person with dementia. It is important to remember that the patient’s actions are not volitional, manipulative, or targeted at you personally, but rather are symptoms of a brain disease. Problems with communication may cause each party to have incomplete information, which, especially in an emergency situation, can cause further difficulties.
Walaszek (2020) created a list of tips for communicating with dementia patients, which includes:
Lesson #3: Tips for Communicating with a Person with Dementia
Dementia is a progressive condition that affects cognition and functioning (e.g. memory loss, difficulty communicating or finding words, confusion and disorientation). Most patients with dementia also experience psychological changes such as personality changes, depression, anxiety and/ or inappropriate behaviour (Walaszek, 2020) (see Fig. 4).

Figure 4: Common Symptoms of Dementia © neofect (2021)
Persons affected by dementia often battle with feelings of fear and insecurity, such as fearing memory loss and thinking skills or ‘loosing who they are’. At later stages, they may not understand what's going on or they feel they're not in control of what's happening around them or to them. All of this can affect their behavior.
These symptoms may make it challenging to communicate with a person with dementia. It is important to remember that the patient’s actions are not volitional, manipulative, or targeted at you personally, but rather are symptoms of a brain disease. Problems with communication may cause each party to have incomplete information, which, especially in an emergency situation, can cause further difficulties.
Walaszek (2020) created a list of tips for communicating with dementia patients, which includes:
- Speaking slowly, clearly, and directly to the patient by using simple words and sentences
- Giving the patient adequate time to respond.
- Do not interrupt, correct, criticize, or argue.
- Break down questions, statements and requests into shorter phrases (e.g., replace a multiple-step request with a sequence of single-step requests).
- Give visual cues and demonstrations along with verbal statements.
- Use written notes as reminders and checklists.
- Be patient
In addition to these points, it is further advisable to set a positive mood for interaction through your whole attitude and body language. Speaking in a pleasant and respectful manner can help with communication as well. To get the patient’s attention it is advisable to limit distractions and noises, e.g. turning off the radio or TV or shutting the door.
Lesson #4: Basics of "Psychological First Aid" in Crisis Situations
When working with people during and after a disaster, it is important to keep in mind that you are working with humans who may have reactions of confusion, fear, anxiety or shock.
In order to reduce this initial distress caused by often traumatic events, Psychological First Aid (PFA) has been developed as an initial disaster response intervention. It helps supporting people during emergencies and offers guidance on delivering psychosocial care in the immediate aftermath of the emergency event. PFA consists of a systematic set of helping actions aimed at reducing initial post-trauma distress and supporting short- and long-term adaptive functioning.
Great strengths of PFA are that it “includes basic information-gathering techniques to help providers make rapid assessments of survivors’ immediate concerns and needs, and to implement supportive activities in a flexible manner” (National Child Traumatic Stress Network (NCTSN) & National Center for PTSD, 2006). PFS also relies on field-tested, evidence-informed strategies that can be provided in a variety of disaster settings.
Important components of PFA are to communicate calmly with an open posture and eye contact, to communicate warmth, i.e. using a soft tone and to establish a relationship with the patient. This can look like introducing yourself, if they do not know you and asking the person what they would like to be called. Help can range from providing physical and emotional comfort to offering practical assistance and information to help survivors address their immediate needs and concerns (National Child Traumatic Stress Network (NCTSN) & National Center for PTSD, 2006). This can be as simple as offering food, water or blankets.
Three basic action principles of PFA are to look, listen and link (see Fig. 5). As crisis situations can change rapidly, it is important to take time – even just a few moments – to look around before offering help. This may be just a quick scan of the situation, but it could give you a chance to be calm, safe and think before you act. Important questions and topics to consider when you look around are safety (What dangers can you see in the environment? Can you enter the scene without harming yourself or others?), people with obvious urgent basic needs (Is anyone critically injured and in need of emergency medical help? Does anyone seem to need rescuing?), and people with serious distress reactions (Where and who are the most distressed people?). “Listening properly to people you are helping is essential to understand their situation and needs, to help them to feel calm, and to be able to offer appropriate help” (World Health Organization (WHO), 2011).
Approach people who may need support respectfully and according to their culture. Ask about people’s needs and concerns, and listen to people and help them to feel calm. This can look like staying close to a person, but not pressuring them to talk. The last action principle revolves around linking people with practical support such as basic needs (e.g. shelter, food) or health services for injuries.
Figure 5: Basic Action Principles of PFA © WHO (2011)
Lesson #5: Top 10 Communication Principles for effective communication with seniors
Czech National Disability Council suggests the following principles:
1. Respect for identity
Lesson #4: Basics of "Psychological First Aid" in Crisis Situations
When working with people during and after a disaster, it is important to keep in mind that you are working with humans who may have reactions of confusion, fear, anxiety or shock.
In order to reduce this initial distress caused by often traumatic events, Psychological First Aid (PFA) has been developed as an initial disaster response intervention. It helps supporting people during emergencies and offers guidance on delivering psychosocial care in the immediate aftermath of the emergency event. PFA consists of a systematic set of helping actions aimed at reducing initial post-trauma distress and supporting short- and long-term adaptive functioning.
Great strengths of PFA are that it “includes basic information-gathering techniques to help providers make rapid assessments of survivors’ immediate concerns and needs, and to implement supportive activities in a flexible manner” (National Child Traumatic Stress Network (NCTSN) & National Center for PTSD, 2006). PFS also relies on field-tested, evidence-informed strategies that can be provided in a variety of disaster settings.
Important components of PFA are to communicate calmly with an open posture and eye contact, to communicate warmth, i.e. using a soft tone and to establish a relationship with the patient. This can look like introducing yourself, if they do not know you and asking the person what they would like to be called. Help can range from providing physical and emotional comfort to offering practical assistance and information to help survivors address their immediate needs and concerns (National Child Traumatic Stress Network (NCTSN) & National Center for PTSD, 2006). This can be as simple as offering food, water or blankets.
Three basic action principles of PFA are to look, listen and link (see Fig. 5). As crisis situations can change rapidly, it is important to take time – even just a few moments – to look around before offering help. This may be just a quick scan of the situation, but it could give you a chance to be calm, safe and think before you act. Important questions and topics to consider when you look around are safety (What dangers can you see in the environment? Can you enter the scene without harming yourself or others?), people with obvious urgent basic needs (Is anyone critically injured and in need of emergency medical help? Does anyone seem to need rescuing?), and people with serious distress reactions (Where and who are the most distressed people?). “Listening properly to people you are helping is essential to understand their situation and needs, to help them to feel calm, and to be able to offer appropriate help” (World Health Organization (WHO), 2011).
Approach people who may need support respectfully and according to their culture. Ask about people’s needs and concerns, and listen to people and help them to feel calm. This can look like staying close to a person, but not pressuring them to talk. The last action principle revolves around linking people with practical support such as basic needs (e.g. shelter, food) or health services for injuries.

Figure 5: Basic Action Principles of PFA © WHO (2011)
Lesson #5: Top 10 Communication Principles for effective communication with seniors
Czech National Disability Council suggests the following principles:
1. Respect for identity
- If we do not have clearly defined rules of addressing a senior in a way other than the one commonly used, we must respect their identity and uniqueness by addressing them by their name or title. Avoid inappropriate, familial or indecent forms of addressing. Very often, we encounter the form of address of a diminished first name, which is possible only if the senior - client agrees with it, or clearly requires it, or it is in accordance with the improvement of their physical or mental condition.
2. Avoid childish conversation
- A senior is not a child. The population sometimes claims that we go back to childhood in old age, but again, this is one of the factors that is not always based on solid and scientifically proven research. Seniors are still adults and we must respect that fact. We should also avoid the childish conversation with clients suffering with dementia or those with Alzheimer's disease or other degenerative diseases
3. Do not devalue the senior's dignity
- Cognitive needs may decrease in old age, but again, this cannot be considered a globally applicable phenomenon. It often happens that communicators underestimate the communication skills of a senior, precisely because of the unverified ability of impaired cognitive functions. If we want to communicate in a different way than commonly used, it is necessary to use available means to verify that the senior really has impaired cognitive functions
4. Respect for the principle of slowing down
- When communicating with a senior, it is necessary to take into account that very often they need a greater time allowance to manage specific tasks, activities, processes that they previously performed without any problems. And this also applies to communication. If we "push" the client - senior, they may get into a situation that is uncomfortable for them and primarily stresses them out, which will significantly affect their quality of life.
5. The principle of repetition
- Even a person of a productive age uses clear, proven formulas to remember information or events. This ability does not disappear with age, it only weakens. Therefore, it is important that we communicate very important or more complex information and data several times when communicating with the senior, or use other communication channels - such as writing such information down and placing it where the senior can easily find it, or verify that the senior has created their own mnemonic aid to remember it
6. Defining possible communication barriers
- The possible communication barrier is not always evident at first glance. As is well known, seniors can suffer from a specific illness or disability, which can limit their ability to communicate and listen effectively, and there is often an accumulation of disabilities. In order for our communication to be at the desired level and to fulfil its purpose, we must identify these barriers (e.g. visual, hearing impairment, etc.) and adjust communication to the given handicap, or rather adapt it.
7. To move in the field of vision of a communicating senior
- The Taro principle is also associated with the requirement for intelligible speech. The senior should be able to see us when we are communicating with them, and we should strive for clear speech. If we know that a senior has impaired visual perception, we should be within their reach and maintain adequate eye contact. We must also not neglect the need to oversee the use of the necessary compensatory aids and resources of any nature
8. Perception of hearing impairment
- Here we very often find ourselves in a situation where if the senior does not hear the information communicated or interprets it in a different context, we raise our voice. A better solution is to eliminate the associated noise (if nearby) and focus more on pronunciation. Again, we should pay attention to the use of compensatory aids
9. Help x independence
- Sometimes we internally feel that the senior is not managing their normal activities and processes and we automatically assume that our help is desirable, necessary, required. The opposite may be true: a senior may feel limited by our good will to help, they may feel underestimated, mentally and physically discriminated. We thus provide so-called unsolicited help, albeit in good faith. None of the help or assistance we provide should be forced.
10. Communication in institutional care
- If a senior becomes a residential care client due to their health or social situation, we must perceive this as a factor that should contribute to maintaining, supporting, improving, stabilising or restoring their quality of life, self-sufficiency, self-confidence, etc. This situation must not be understood as partial or complete loss of communication or other functions.
Some of the rules listed here may seem obvious to us, but in communication with seniors we very often commit communication stereotypes. Usually, we do not consciously apply these "dormitory" syndromes, we only try to "refine" communication and forget that seniors have the same communication premises, which should simply be adapted to their specific needs.
These communication principles are very often associated with a way of communication, where we can talk about the phenomenon of power, which can manifest itself in authoritative decision-making, from which communication errors arise:
1. One-way communication: lack of dialogue, reluctance, inability to listen
2. Absence of feedback: failure to verify understanding of the information provided
3. Devaluation behaviour: insult to the senior
4. Insufficient authenticity of the message: confusing message, contradictions in the conversation, discrepancy between verbal and non-verbal communication, which can cause confusion and incomprehensibility to the senior
5. Communication manipulation: use of words incomprehensible to the senior, words distorted, expressions that seniors do not normally encounter
6. Non-acceptance of the dynamics of communication time: every communication with a senior requires its own time, it is not possible to plan "for minutes"
In order to eliminate mistakes, it is desirable to use the rules, techniques and methods of active listening that are valid for social communication and it is in our power to adapt them to our target group - seniors:
1. Encouragement (yes, tell me, I understand…)
2. Clarification (you mean it like that, it’s like this…)
3. Mirroring (verifying that the listener has understood the speaker)
4. Paraphrasing ("retelling" the communicated content in your own words to the listener to check the level of understanding of the information)
5. Summary (summary of reported data)
6. Appreciation (communicator support) (NRZP, 2006)